

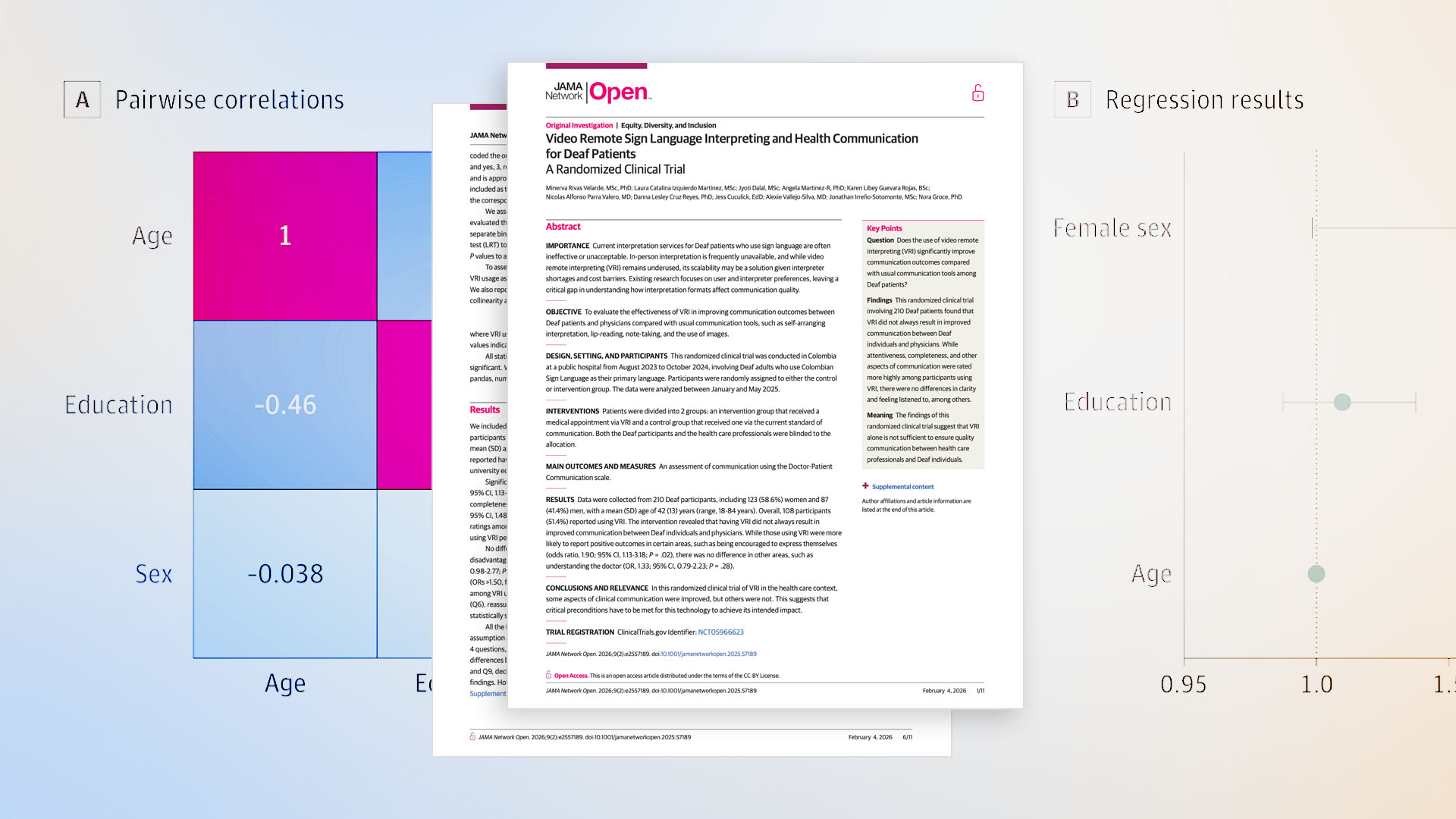
A randomized clinical trial (RCT) published this month in JAMA Network Open examined whether video remote interpreting (VRI) improves communication outcomes for Deaf patients during medical consultations. The study, conducted in Colombia with 210 Deaf adults, is the first of its kind to test VRI’s impact on doctor-patient communication using a rigorous RCT design.
The results were mixed — and that’s precisely what makes them important.
VRI improved communication in several meaningful areas. Patients reported:
- Feeling more encouraged to express themselves;
- Receiving more thorough physical examinations;
- Being given more complete information;
- And being more involved in clinical decision-making.
But, in the study, VRI made no significant difference in other critical domains — patients using VRI were no more likely to feel that the doctor listened carefully, that explanations were clear, that the doctor understood them, or that their concerns were fully addressed.
The researchers’ conclusion deserves attention: VRI alone is not sufficient to ensure quality communication. Critical preconditions — interpreter training, quality governance, and user readiness — must be in place for the technology to achieve its intended impact.
For anyone working in language access, this isn’t surprising. But having it validated in a peer-reviewed RCT in a respected medical journal gives us a foundation to have important conversations about what actually drives communication quality in healthcare.
Technology Is Necessary, Not Sufficient
The healthcare industry has invested heavily in remote interpreting technology over the past decade, and for good reason. VRI expands access, reduces wait times, and makes interpretation available in settings where in-person interpreters simply aren’t feasible. These are real, measurable benefits.
But the study illustrates a pattern that practitioners on the ground already recognize: deploying the technology is only part of the equation.
When patients report that VRI helped them feel more encouraged to speak and more involved in decisions — but did not help them feel understood or confident in the physician — that gap points squarely at the human layer of the interaction, not the technical one.
In other words, the screen worked. The connection was made. But the quality of what happened through that connection varied. And the variable that governs that quality isn’t bandwidth or screen size. It’s the interpreter.
Interpreter Quality Is the Intervention
The study’s authors point to limited health literacy and prevailing mistrust toward interpretation personnel as factors that likely shaped participant responses. They note weak training and governance structures for interpreters in the study’s context, and describe an environment where interpreter qualifications are inconsistent and not subject to standardized oversight.
This is a critical insight because it reframes the intervention.
The question isn’t simply “does VRI work?” — it’s “under what conditions does VRI produce better outcomes?” And the evidence increasingly points to the same answer: trained, qualified interpreters operating within structured quality assurance systems are what turn a video connection into an effective clinical communication tool.
When interpreters are specifically trained in medical terminology, clinical workflows, ethical standards, and culturally sensitive communication, the technology has something meaningful to deliver. Without that foundation, even a perfectly functioning VRI system is transmitting a suboptimal interaction.
The Implications Extend Beyond Sign Language Interpretation
While this study focused on Colombian Sign Language interpretation for Deaf patients, the underlying dynamics are directly relevant to ASL and spoken-language remote interpretation in U.S. healthcare settings. The principle is the same: the technology is the delivery mechanism, but interpreter preparation and governance are what determine whether the communication actually succeeds.
Health systems evaluating or managing remote interpreting services — whether for spoken or signed languages — should be asking the same questions this study raises. Not just “do we have access to interpretation?” Consider the following:
- “Are the interpreters who connect through our systems trained specifically for healthcare?”
- “Are they subject to ongoing quality assurance?”
- “Do patients and clinicians trust the interaction?”
The study’s finding that VRI improved some communication domains but not others is a useful lens for any organization assessing the performance of their language access program. Where outcomes are inconsistent, look at the qualification, training, and oversight of the interpreters connecting through it.
.png)
Important Context
A few caveats are worth noting. This study was conducted in Colombia, a country where interpreter training infrastructure, regulatory frameworks, and digital access patterns differ meaningfully from those in the United States. The researchers acknowledge that limited health literacy among the Deaf population and weak governance structures for interpreters likely influenced results. These conditions are not identical to the U.S. healthcare environment, where interpreter qualification standards, while variable, are generally more established.
That said, the core finding — that technology without adequate interpreter preparation leaves critical communication gaps — is not context-dependent. It’s a principle that holds true regardless of geography, language modality, or healthcare system design. And it’s consistent with a growing body of evidence showing that interpreter quality, not just interpreter availability, is what drives clinical outcomes.
What This Means for Health System Leaders
For health systems investing in or evaluating remote interpreting services, this study reinforces several priorities that should be non-negotiable:
Interpreter training standards matter more than connection speed. A sub-20-second average speed to answer is important — but only if the interpreter who connects is trained in medical terminology, clinical ethics, cultural sensitivity, and the specific workflows of healthcare delivery. Sourcing decisions should weigh interpreter qualifications at least as heavily as access metrics.
Structured quality assurance is not optional. The study highlights the consequences of operating without governance mechanisms for interpreter quality. Health systems should require evidence of structured QA programs — ongoing training, performance monitoring, and accountability — from any language access partner.
Healthcare-only interpreters reduce variability. Interpreter pools that serve multiple industries — not exclusively healthcare — introduce quality variability that directly affects patient communication. The evidence supports working with interpreters who are trained exclusively for healthcare, understand clinical contexts, and can navigate the specific demands of medical conversations.
Evaluate outcomes, not just utilization. Minutes used and sessions completed tell you whether interpretation is being accessed. They don’t tell you whether communication is actually succeeding. Health systems should be measuring the quality of interpreted encounters through patient feedback, clinician experience data, and clinical outcome metrics, not just volume.
The Bigger Picture
Remote interpreting technology has expanded language access in ways that would have been unimaginable a generation ago. That progress is real and worth recognizing. But this study is a timely reminder that access and quality are not the same thing.
The health systems that will deliver the best communication outcomes for patients with language access needs are not necessarily the ones with the most sophisticated technology. They are the ones that pair effective technology with rigorously trained, healthcare-specialized interpreters, supported by structured governance and continuous quality improvement.
That’s not a technology problem. It’s a standards problem, a training problem, and a sourcing problem. And it’s one that health system leaders have the ability — and the responsibility — to solve.
References
Rivas Velarde M, Izquierdo Martinez LC, Dalal J, et al. Video Remote Sign Language Interpreting and Health Communication for Deaf Patients: A Randomized Clinical Trial. JAMA Network Open. 2026;9(2):e2557189.
doi:10.1001/jamanetworkopen.2025.57189
About the Author







